Biological effects & Radiation units
Learning Objectives
- Benefits and detriments of ionising radiation
- Development of radiation protection
- Quantities and units used in radiation protection
- Deterministic and stochastic effects of ionising radiation
- Quantitation of radiation risk
- Principles of radiation protection
Ionising Radiation
Benefits
In 1896 a German physics professor, William Röntgen, found a new kind of ray which he called the ‘x-ray’. There was an immediate worldwide excitement and Henri Becquerel quickly discovered radioactivity a year later. Then on 26 December 1898, Marie Curie and her husband Pierre announced the existence of a new element, which they name ‘radium’. They were fascinated by its effects on destroying tumour cells faster than the surrounding healthy cells. And within a few years systems were being devised to treat cancer.
Early Radiology
In the beginning radiographs were initially made onto glass photographic plates, film wasn’t introduced until 1918 thanks to George Eastman. Right from the start x-rays were used as a therapy, for ailments such as skin lesions.
Early Radiotherapy
Many early radiologists tested the strength of their radiotherapy machines by using their own arms. If their skin turned pink then this was estimated to be the correct ‘erythema dose’ as they called it. Unfortunately, unaware at the time a lot of them ended up developing leukaemia from exposing themselves to so much radiation.
Alternative Therapies
Soon people started to think that radiation was a ‘wonder cure’ for everything and a whole host of alternative therapies arose:
- Quack cures: a whole host of products were created including radium toothpaste and radium suppositories ‘for restoring sexual power’
- Radium bread: bread was even made with radium water
- Fluoroscopic shoe fitting: fluoroscopy screens were used to see if shoes were the right size
- Thermal spring, (Pammukule, Turkey) is thought to have healing powers
Detriments
However with the increased popularity of radiation, it was soon discovered that an excess of radiation would not cure cancer and other ailments but end up having a detrimental effect on human health.
Eyes irritation
One of the first warnings of possible adverse side effects came from Thomas Edison, William J. Morton and Nikila Tesla who all reported independently of one another, eye irritations from experimentation from x-rays and fluorescent substances.
Skin pain swelling burns
Elihu Thomson, an American physicist, deliberately exposed one of his little fingers to an x-ray tube for several days (half an hour a day) and ended up experiencing pain, swelling, stiffness, erythema and blistering.
Development of Radiation Protection
As it became more and more apparent that radiation is harmful when used incorrectly, safety measures were slowly introduced to try and reduce the harmful effects of radiation.
Protective Clothing 1920
People start to use protection such as lead clothing.
Regulations introduced 1921
British x-ray and Radium committee introduces regulations:
- No more than 7 working hours / day
- Sundays and 2 half days off per week
- As much leisure time as possible spent out of doors
- Annual holiday of 1 month or 2 fortnights
- Nurses in x-ray and radium departments should not work elsewhere
First International Congress of Radiology 1925
Is a meeting of radiologists, where they can exchange their ideas and harmonies the international standards and practice of radiology. With the first meeting in London in 1925, it is still running today with its 29th meeting in Buenos Aires in 2016.
Röntgen unit introduced 1931
The Röntgen (R) is the amount of radiation to produce a certain amount of ionisation in a given volume of air.
First dose limit 1934
First dose limit. ICRP recommends a tolerance dose limit of: 0.2 rad/day (~ 500 mSv/y)
Stochastic effects 1950
Reports of increases in leukaemia and other cancers from bomb survivors and therapy patients. Risk extrapolates to zero dose (no safe dose).
Quantities & Units of Radiation
As soon as it became understood that radiation is harmful when not used carefully, ways of measuring its dose were calculated and here are three different types:
1. Absorbed dose Gy
This reflects the amount of energy that radioactive sources deposit in medium (e.g. water, tissue, air) through which they pass. The absorbed dose can be calculated with the following equation:
Units are in Grey (Gy, mGy, cGy), 1 grey = 1 joule per kg. Different absorbed doses can lead different effects.
Bone marrow syndrome 1 - 10 Gy
With a radiation exposure 1 - 10 Gy, symptoms can include:
- Leucopenia (reduction in the number of white blood cells)
- Thrombocytopenia (lower platelet count)
- Haemorrhage (escape of blood from a ruptured blood vessel)
- Infections
A therapy for this amount of exposure is using symptomatic transfusions of leucocytes and platelets, bone marrow translation and growth stimulating factors. Prognosis is excellent to uncertain with survival rates ranging from 10% to 100%.
Gastrointestinal Problems 10 - 50 Gy
With a radiation exposure 10 - 50 Gy, symptoms can include:
- Diarrhoea (the shits)
- Fever (raised body temperature)
- Electrolytic imbalance (an imbalance of electrolytes such as sodium, potassium, urea etc)
Palliative care would be recommended, this may include controlling the diarrhoea and fever as well as replacing lost electrolytes. If you are lucky some morphine. Prognosis is very poor, survival rate is 10%.
Central nervous syndrome > 50 Gy
With a radiation exposure greater than 50 Gy, you can expect to see the following symptoms:
- Cramps (painful involuntary contraction of muscle)
- Tremor (involuntary shaking)
- Ataxia (impaired movement)
- Lethargy (lack of energy)
- Impaired vision
- Coma (a prolonged state of deep unconsciousness)
Symptomatic treatment would be advised to ease the above symptoms. Prognosis is hopeless, with the survival rate being 0%.
Lethal dose 50/30
Is the dose which would cause death to 50% of the population in 30 days. Its value is about 2-3 Gy for humans for whole body irradiation.
Relative Biological Effectiveness RBE
RBE is the ratio of biological effectiveness of one type of ionising radiation relative to another, given the same amount of absorbed energy. See the graph below for a few examples:
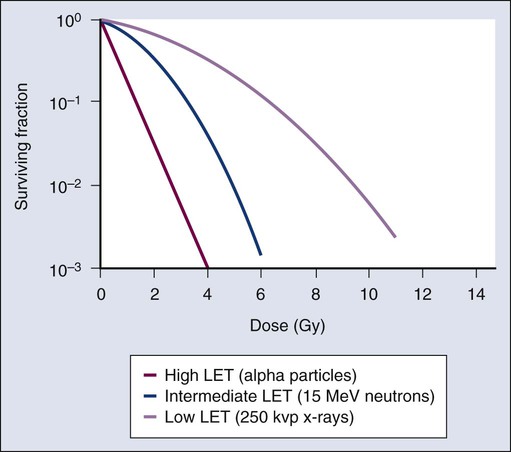
Note: LET stands for Linear Energy Transfer
2. Equivalent dose Sv
This is a measure of the radiation dose to tissue where an attempt has been made to allow for the different relative biological effects of different types of ionising radiation. It is used to assess how much biological damage is expected from an absorbed dose, as different types of radiation have different damaging properties. Equivalent dose is calculated with the following equation:
Equivalent dose is measured in Sieverts (Sv, mSv) but REM (Roentgen Equivalent in Man) is commonly used as well, where 1 Sv = 100 REM.
3. Effective dose Sv
This determines how dangerous an individual’s exposure to radiation can be, by taking into consideration not only the nature of the incoming radiation but also the sensitives of the body parts affected.
Effective dose is measure in Sieverts (Sv, mSv) and below are some common tissue weighting factors:
| Tissue | Wr | $\sum$ Wr |
|---|---|---|
| Bone marrow, Brest, Colon, Lung, Stomach | 0.12 | 0.60 |
| Gonads | 0.08 | 0.08 |
| Bladder, Oesophagus, Liver, Thyroid | 0.04 | 0.16 |
| Bone surface, Brain, Salivary Glands, Skin | 0.01 | 0.04 |
| Remainder Tissue | 0.12 | 0.12 |
A Few Calculations
Here are a few example calculations using the above principles:
- Whole body absorbed dose of 5 Gy = Whole body effective dose of 5 Sv
- Thyroid absorbed dose of 5 Gy = Whole body effective dose of 5 x 0.04 = 0.2 Sv
- Thyroid, lung & heart absorbed dose of 5 Gy = (5x0.4) + (5x0.12) + (5x0.12) = 1.4 Sv
Biological Effects of Radiation
Ionisation is the process by which an atom or a molecule acquires a negative or positive charge by gaining or losing electrons to form ions, and this is often caused by radiation. Ionising radiation can have potentially disastrous effects on our body at a cellular level, causing radiochemical damage by either direct or indirect action:
1. Direct action
Direct action occurs when alpha particles, beta particles or x-rays create ions which physically break the sugar phosphate backbones or the weak hydrogen bonds holding together the base pairs of the DNA. However, heavy charged particles (alpha particles) have a greater probability of causing direct damage compared to the low charged particles (x-rays) which cause most of the damage by indirect effects.
2. Indirect action
Indirect action is when ionising radiation effects other biological molecules such as water. It can impair or damage cells indirectly by creating free radicals which are highly reactive due to the presence of unpaired electrons on the molecule.
Radical Formation
H2O + Radiation H2O+ + e-
Free radicals may form compounds, such as hydrogen peroxide, which could initiate harmful chemical reactions within the cells.
Recombinant compounds
H2O OH H2O2
Following these chemical changes cells may undergo a variety of different processes.
Reparation after exposure
Once damaged DNA usually usually repairs itself through a process called excision, this process has three main steps:
- Endonucleases cut out the damaged DNA
- DNA polymerase resynthesises the original DNA
- DNA ligase repairs the sugar phosphate backbone
Unfortunately this method is not fool-proof and sometime DNA is incorrectly repaired. This can either lead to cell death or a mutation (either a substitution or a frameshift). And occasionally this could lead to the formation of cancer.
Forms of damage
With any exposure to radiation there is a risk that damage can occur and there are three main types:
- Genetic Damage
- Somatic Damage (formation of cancer)
- Teratogenic Damage (malformation of an embryo)
Classification of effects
The biological effects of radiation can be classified in two ways, deterministic and stochastic:
Deterministic direct effect
Deterministic effects describe a cause and effect relationship between radiation and some side-effects. They are also called non-stochastic effects to contrast their relationship with the chance-like stochastic effects, e.g. of cancer induction.
Deterministic effects have a threshold below which, the effect does not occur. The threshold may be very small and may vary from person to person. However, once the threshold has been exceeded, the severity of an effect increases with dose. Some examples of deterministic effects include:
- Skin erythema 2-5 Gy
- Irreversible skin damage: 20-40 Gy
- Hair loss: 2-5 Gy
- Sterility 2-3 Gy
- Cataracts: 5 Gy
- Lethality (whole body): 3-5 Gy
- Fetal abnormality: 0.1-0.5 Gy
Note: Doses given at absorbed dose
| Tissue | Effect | Threshold Dose (Sv) |
|---|---|---|
| Testes | Sterility | 0.15 (temp) |
| Ovaries | Sterility | 3.5-6 (perm) |
| Lens | Opacities (Cataract) |
0.5-2 5 |
| Bone marrow | Depression of haematopoeisis | 0.5 |
Stochastic occur by chance
Stochastic effects occur by chance. Cancer induction as a result of exposure to radiation occurs in a stochastic manner aS there is no threshold point and risk increases in a linear-quadratic fashion with dose. This is known as the linear-quadratic no threshold theory. Although the risk increases with dose, the severity of the effects do not; the patient will either develop cancer or they will not.
Determining Stochastic Risk
You can determine stochastic risk by creating epidemiological studies using risk data form:
- Occupational risk data such as dial painters, uranium miners, early radiologists
- Medical risk data such using fluoroscopy to diagnose TB, mammography (breast screening), therapy of ankylosing spondylitis (spinal arthritis), ringworm or artificial menopause.
- Fallout risk data from atomic bombs (Hiroshima and Nagasaki) and other nuclear disasters such as Chernobyl.
You can quantify this risk, for example the medical radiation risk (at 5% per Sv) in the table below:
| Procedure | Effective Dose (mSv) | Risk (per million) |
|---|---|---|
| Dental OPG | 0.08 | 4 |
| CXR | 0.03 | 2.5 |
| Abdom. X-ray | 2.0 | 100 |
| IVU | 4.0 | 200 |
| Barium Enema | 8.0 | 400 |
| CO-58 B12 | 0.2 | 10 |
| Tc-99m V/Q | 1.0 | 50 |
| Tc-99m Bone | 3.0 | 150 |
| Abdo Ct | 15.0 | 750 |
Framework for Radiation Protection
The following are three fundamental principles of radiation protection, taken from the ICRP (International Commission on Radiological Protection) system:
Justification Radiation is harmful
The principle of justification requires that any decision that alters the radiation exposure situation should do more good than harm; in other words, the introduction of a radiation source should result in sufficient individual or societal benefit to offset the detriment it causes.
Optimisation Stochastic effects
The principle of optimisation requires that the likelihood of incurring exposures, the number of people exposed and the magnitude of their individual exposure should all be kept as low as reasonably achievable, taking into account economic and societal factors. In addition, as part of the optimisation procedure, the ICRP recommends that there should be restriction on the doses to individuals from a particular source and this leads to the concept of dose constraints.
Limitation Deterministic effects
The third principle of the ICRP’s system of protection is that of dose limitation. This principle requires that the dose to individuals from planned exposure situations, other than medical exposure of patients, should not exceed the appropriate limits recommended by the Commission.
Example Problem
Following a malfunction in the cooling circuit of an experimental nuclear reactor there was a catastrophic failure leading to an explosion. A monitoring station on the periphery of the reactor site at a distance of 100m from the reactor showed that the whole body absorbed dose to an individual at that point would have been 20 Gy from the initial radiation burst after the explosion. Other monitoring instruments indicated that the radiation in the burst was comprised 70% gammas and 30% neutrons.
Material vaporised during the explosion entered the atmosphere where it was distributed widely by the prevailing Westerly wind. Monitoring stations at 500m from the reactor recorded the absorbed dose to the lungs following inhalation of particulates from the plume. These particulates comprised 90% gamma-emitting isotopes and 10% alpha-emitting isotopes.
In the direction of the wind the total lung absorbed dose would have been 10 Gy. Individuals at the same distance from the reactor but at 900 to the wind direction would have received only 30% of this absorbed dose to the lungs. Individuals at 500m and in the opposite direction to the wind would receive no absorbed dose from particulates in the plume.
Make an estimate of the percentage increase in cancers expected in populations at distances of 1000, 2000 and 3000m from the reactor at the four cardinal points of the compass. Fully describe each step taken in reaching your answers.
You can assume that the inverse square law applies to both the initial radiation burst and the subsequent distribution of the plume. Also assume that the radiation weighting factor for neutrons is 2 and for alpha particles, 20. The only significant organ dose following inhalation is to the lungs.
Solution
Solution coming soon
Written by Tobias Whetton